TALVEY® mechanism
of action
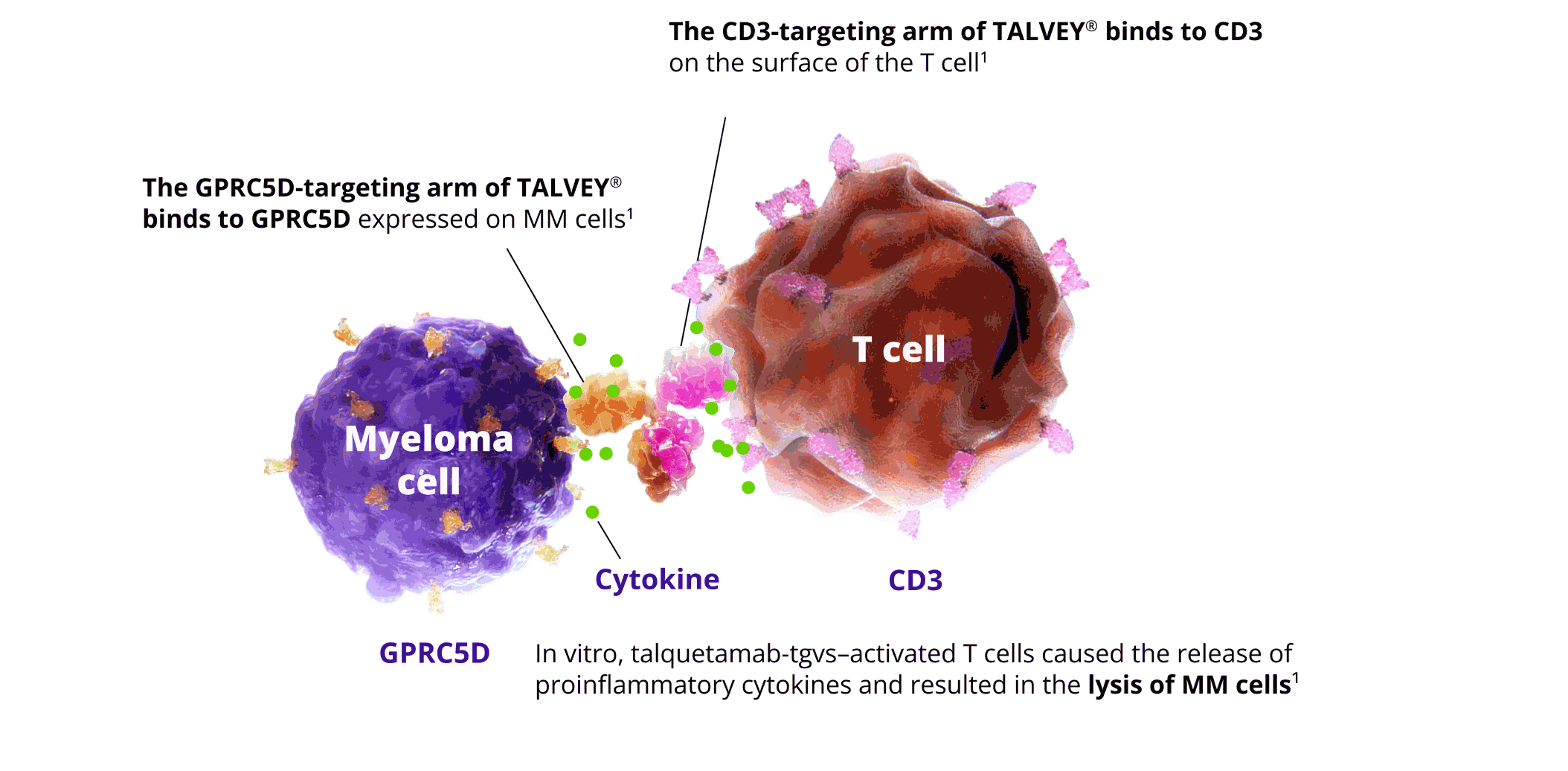
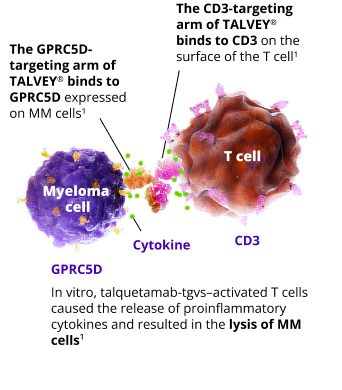
TALVEY® induces the lysis of MM cells by activating the immune system via GPRC5D × CD31
- In research that examined GPRC5D mRNA expression in malignant cells, GPRC5D mRNA was found to be substantially expressed in MM cell lines1,4
- This finding led to the commitment of Johnson & Johnson and its affiliates to pursue the development of a
GPRC5D-targeting therapy for MM5
GPRC5D expression is strong
in myeloma cells and weak to nonexistent in healthy plasma cells6–9
- GPRC5D is expressed on the surface of MM cells and nonmalignant plasma cells. It is also expressed on healthy tissues such as epithelial cells in keratinized tissues of the skin and tongue1,6–8,10,11
- GPRC5D is expressed in a broad range of patients with MM who vary according to disease staging, cytogenetic abnormalities, gender, and age6
- GPRC5D expression is independent of other targets, including BCMA4
With emerging research, GPRC5D has been identified as a target with a potential role in cancer treatment4,6
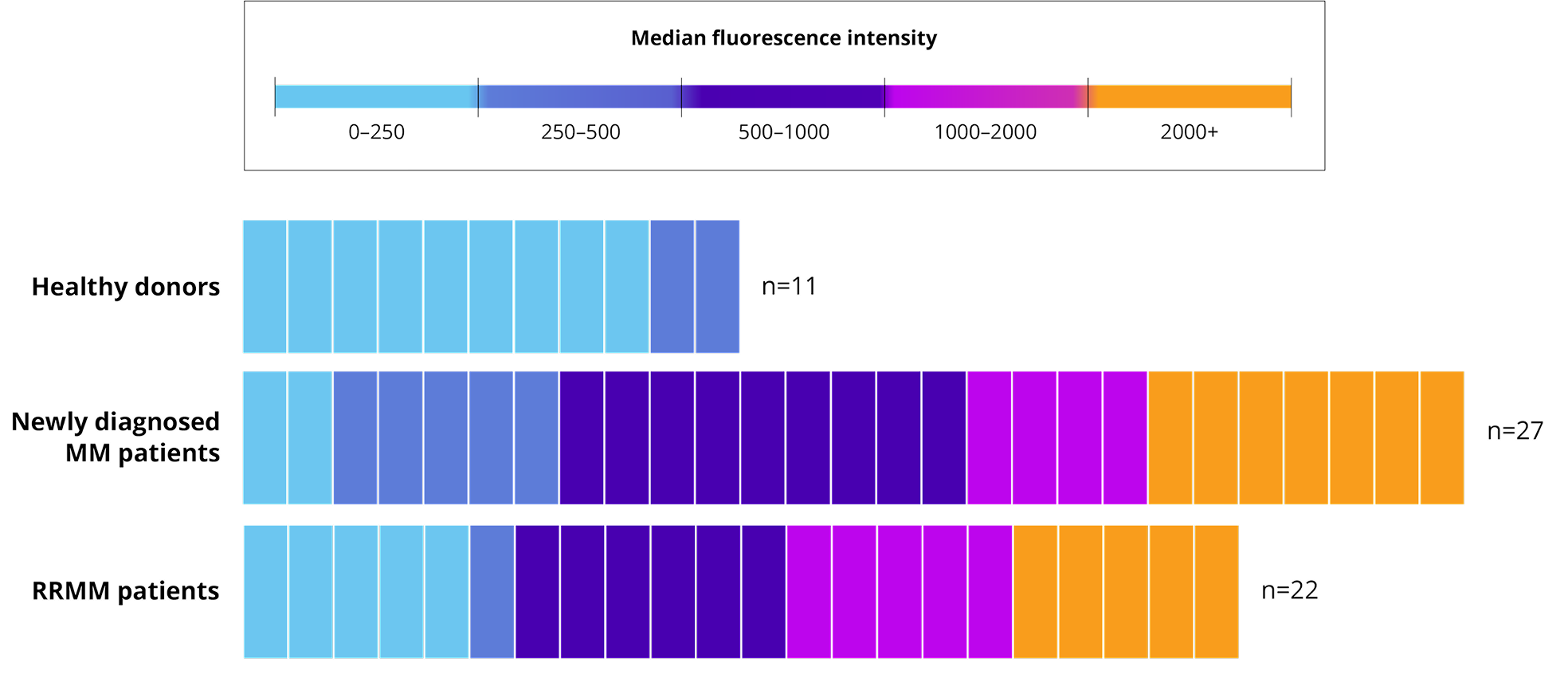
In a study intended to increase understanding of GPRC5D expression, flow cytometry analysis was performed on fresh bone marrow samples and median fluorescence intensity was used to assess the cell surface expression of GPRC5D in MM cells in newly diagnosed MM patients, daratumumab-naïve RRMM patients, and plasma cells obtained from age-matched healthy donors.8
Higher GPRC5D cell surface levels were detected on MM cells (from newly diagnosed MM and RRMM patients) vs normal plasma cells from healthy donors.
GPRC5D expression in
various donors8

GPRC5D expression has limited to no known impact on healthy B cells and is prominently found on malignant MM cells6–9
GPRC5D expression is not detected in early B-cell lines, such as pro-B cells and early progenitor cell lines.


The National Comprehensive Cancer Network® (NCCN®) recommends introducing different drugs/drug classes for the treatment of RRMM12
For RRMM, the NCCN recommends new regimens, including drugs or drug classes that patients have not been previously exposed to, or exposed to >1 line prior.
Different targets may help address treatment resistance and avoid re-exposure to previous targets.4,6,13
NCCN recommendation12
CATEGORY 2A
NCCN
PREFERRED
in Oncology (NCCN Guidelines®) recommend talquetamab-tgvs (TALVEY®) as an NCCN Category 2A preferred treatment option for multiple myeloma after at least
4 prior therapies, including an
anti-CD38 monoclonal antibody, a proteasome inhibitor, and an immunomodulatory agent.
NCCN makes no warranties of any kind whatsoever
regarding their content, use or application and disclaims any responsibility for their application or use in any way.
BCMA, B-cell maturation antigen; CD, cluster of differentiation; FDA, U.S. Food and Drug Administration; GPRC5D, G protein-coupled receptor class C group 5 member D; MM, multiple myeloma; mRNA, messenger ribonucleic acid; RRMM, relapsed or refractory multiple myeloma.
Watch how TALVEY®
targets GPRC5D
The need for new
treatments in MM
See TALVEY®
efficacy data
- TALVEY® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
- U.S. FDA approves TALVEY® (talquetamab-tgvs), a first-in-class bispecific therapy for the treatment of patients with heavily pretreated multiple myeloma. Janssen Biotech, Inc. Updated August 10, 2023. Accessed October 1, 2025. https://www.janssen.com/fda-approves-talveytmtalquetamab-tgvs-first-class-bispecific-therapy-treatment-patients-heavily
- Einsele H, Moreau P, Bahlis N, et al. Adv Ther. 2024;41(4):1576–1593. doi:10.1007/s12325-024-02797-x
- Smith EL, Harrington K, Staehr M, et al. GPRC5D is a target for the immunotherapy of multiple myeloma with rationally designed CART cells. Sci Transl Med. 2019;11(485):eaau7746.
- Pillarisetti K, Edavettal S, Mendonça M, et al. A T-cell-redirecting bispecific G-protein-coupled receptor class 5 member D x CD3 antibody to treat multiple myeloma. Blood. 2020;135(15):1232–1243.
- Atamaniuk J, Gleiss A, Porpaczy E, et al. Overexpression of G protein-coupled receptor 5D in the bone marrow is associated with poor prognosis in patients with multiple myeloma. Eur J Clin Invest. 2012;42(9):953–960.
- Kodama T, Kochi Y, Nakai W, et al. Anti-GPRC5D/CD3 bispecific T-cell-redirecting antibody for the treatment of multiple myeloma. Mol Cancer Ther. 2019;18(9):1555–1564.
- Verkeij CPM, Broekmans MEC, van Duin M, et al. Preclinical activity and determinants of response of the GPRC5DxCD3 bispecific antibody talquetamab in multiple myeloma. Blood Adv. 2021;5(8):2196–2215.
- Hammons L, Szabo A, Janardan A, et al. The changing spectrum of infection with BCMA and GRPC5D targeting bispecific antibody (bsAb) therapy in patients with relapsed refractory multiple myeloma. Haematol. 2024;109(3):906–914.
- Inoue S, Nambu T, Shimomura T. The RAIG family member, GPRC5D, is associated with hard-keratinized structures. J Invest Dermatol. 2004;122(3):565–573.
- Lancman G, Sastow DL, Cho HJ, et al. Bispecific antibodies in multiple myeloma: present and future. Blood Cancer Discov. 2021;2(5):423–433.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma Version 2.2026. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed December 1, 2025. To view the most recent and complete version of the guideline, go on line to NCCN.org.
- Mateos MV, Weisel K, De Stefano V, et al. LocoMMotion: a prospective, non-interventional, multinational study of real-life current standards of care in patients with relapsed and/or refractory multiple myeloma. Leukemia. 2022;36(5):1371–1376.